Swiss Trial of Decompressive Craniectomy versus Best Medical Treatment of Spontaneous
Supratentorial Intracerebral Hemorrhage: A Randomized Controlled Trial.
Please find more Information on www.clinicaltrials.gov.
Download Leaflet
Synopsis
Treatment of intracerebral hemorrhage (ICH) is the major unresolved issue of acute stroke treatment.
Introduction
Spontaneous intracerebral hemorrhage (ICH) is a major public health problem affecting 2 million people worldwide each year. It is a devastating disease; up to half of the affected patients die within 30 days and the majority of survivors are permanently handicapped.
Why is ICH so devastating?
ICH is the most severe form of stroke. The hemorrhage damages the brain both directly, by destruction of brain tissue, and indirectly by increasing the pressure within the brain. Previous trials have investigated surgical removal of the hematoma. The results were disappointing and the two most recent, carefully performed and important trials (STICH and STICH II) failed to show a benefit after surgical removal of the hematoma. Surgical removal of the hematoma is thought to be ineffective due to additional trauma to the brain. Therefore new concepts are urgently needed to find treatment solutions for this devastating disease.
New concept
Decompressive craniectomy decreases intracranial pressure without further damage to the vulnerable brain. During this procedure the bone of the skull is removed, enabling the brain to expand and thereby reducing intracranial pressure. Decompressive craniectomy is a well-established treatment in patients with large ischemic strokes (major trials: DESTINY, HAMLET, DECIMAL).
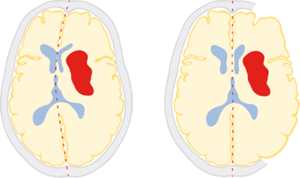
Schematic drawing of hematoma (red) and space-occupying effect before (left) and after decompressive craniectomy (right)
Neurocenter Bern
The Neurocenter Bern is a leading international neurovascular center with the largest number of highly-specialized interventions in Switzerland, including the endovascular clot retrieval after ischemic stroke. In a combined effort between centers in Bern and Geneva, the new treatment concept of decompressive craniectomy after intracerebral hemorrhage has already been successfully applied and results have been published in a major international journal (Stroke) in 2012. This Swiss trial showed that the new treatment is feasible and safe. This trial showed promising effects with regard to mortality and outcome. Based on these results and lively discussions among specialists in Switzerland, we planned to conduct a prospective randomized trial on this new treatment concept.
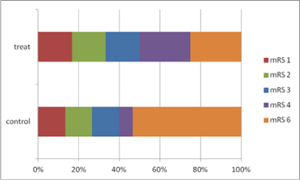
The figure shows outcome (as fractions of 100%) of patients per treatment group as displayed by the modified Rankin Scale (mRS). Lower modified Rankin Scale scores indicate a better outcome (Fung et al. 2012).
SWITCH – the protocol
Aim of the study
The primary aim of this trial in patients with acute intracerebral hemorrhage (ICH) is to show that best medical therapy plus decompressive craniectomy (DC) is superior to best medical therapy alone with respect to the morbidity and mortality of the patients.
Study Protocol
The study will be conducted in major European stroke centers.
Key Inclusion Criteria
- Age: ≥18 to ≤75 years
- Acute stroke syndrome due to a spontaneous ICH
- Haemorrhage into basal ganglia, or thalamus that may extend into cerebral lobes, ventricles or subarachnoid space
- Glasgow coma scale (GCS) <14 and >7
- NIHSS ≥10 and ≤30
- Surgical treatment within 72 hours after ictus
- Volume of hematoma ≥30ml and ≤100ml
Key Exclusion Criteria
- Intracranial aneurysm, brain arteriovenous malformation, brain tumor, brain trauma, stroke thrombolysis
- Cerebellar or brainstem hemorrhage
- Exclusive lobar hemorrhage
- Moribund patients (GCS 3-7)
Treatment Groups
SWITCH will compare early decompressive craniectomy (DC) plus best medical treatment versus best medical treatment alone. All patients in the treatment group will receive a decompressive craniectomy (DC) according to our previously published guidelines. Best medical treatment for both groups is consistent with the current American Heart Association/American Stroke Association (AHA/ASA) guidelines.
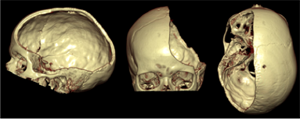
3D-computed-tomography (CT) reconstruction of the skull after decom- pressive craniectomy from three different perspectives
Outcome
The primary outcome is the composite of mortality or dependency at 6 months after treatment (mRS 5 and 6).
Secondary outcome parameters will be: – Mortality – Health-related quality of life (HRQoL) – Neurological impairment (National Institute of Health Stroke Scale) – Complication rate
Sample Size / duration of the trial
As shown in our recent feasibility study (Fung et al. 2012) the proportion of patients with an unfavourable outcome (mRS 5-6) was 0.53 in the control group. Thus, a total sample size of 300 patients will provide over 82% power at a two-sided α level of 0.05 to detect a relative risk reduction of 33% using a Chi-squared test. With 4 major stroke centers participating in Switzerland (Bern, Geneva, Lucerne, Lugano) and sites across 6 European countries (Germany, Austria, Spain, the Netherlands, France and Finland), it is clearly feasible to conduct this trial in the planned time period. Randomization of the patients started in October 2014 and will end in September 2020. After completion of the follow-up period of 6 months, the primary outcome data will be collected in March 2021, with publication of the results anticipated in summer 2021.
Financing
The Swiss National Science Foundation has approved a grant over CHF 520.000 in September 2013. In addition funds were granted from the Swiss Heart Foundation (CHF 100.000) and Inselspital Bern (CHF 80.000).
“What others think”
The idea of using decompressive craniectomy for treatment for ICH is increasing throughout the neurosurgical and neurological community. Shortly after publication of our preliminary results in “Stroke” last year, three new studies were published focusing on decompressive craniectomy in ICH. In addition, our results were reported in the non-scientific media, which should help to improve awareness of this devastating condition.
Discussion
Here is what literature says about our concept:
“I really would like to see one more trial — the trial of decompressive craniectomy for intracerebral hemorrhage”
—Prof. Dr. W. Hacke, meeting of the German Society for Neurology and Neurosurgery in Mannheim 2010.
“These findings suggest that a randomized controlled trial of decompressive craniectomy after ICH is warranted.”
—J Ellitot et al., London, in Anesthesie & Analgesia, 2010
“…preliminary data supports the need for better controlled studies addressing the role of this (hemicraniectomy) surgical technique in ICH patients.”
—Rincon et al., New Jersey, in Current Opinion in Neurology, 2010
“Further evaluation of this method to reduce mortality in ICH patients is warranted.”
—Omary et al., Israel, in Journal of Molecular Neuroscience, 2013
“Large randomized controlled trials are needed to further investigate the therapeutic value of DHC (decompressive hemicraniectomy) in ICH”
—Heuts et al., New York, in Journal of Neurosurgery Focus, 2013
“… but DC ameliorates the mass effect exerted by the ICH plus the perihematomal edema (PHE).”
—Fung et al., PLoS One, 2016
“… Edema growth is an important Treatment target for strategies to improve Patient outcome.”
—Wu et al., Stroke, American Heart and Stroke Association, 2017
Endorsement
The SWITCH- trial has been endorsed by the Stroke Alliance For Europe (SAFE).
![]()